
Decompression Myths Part 2
By: Mark Powell
In the last article I looked at some of the reasons why we have myths in general and also at some of the broad myths relating to decompression. In this second article I am going to be much more specific and focus on one particular area. I am going to consider two common myths about safety stops.
MYTH – It doesn’t matter if you miss a safety stop
The first myth is that safety stops don’t really matter. I’m sure you have all heard divers on the boat saying that they missed their safety stop but it doesn’t matter as they are optional. After all, in the last article I stated that a no-stop dive is one where you can ascend directly to the surface without needing to stop. Safety stops are often described as optional rather than mandatory stops. This is all true but that doesn’t mean that safety stops don’t matter. The first reason why this is the case is that the traditional approach assumes that there is a hard and fast line between having bubbles and not having bubbles. This limit represents the maximum amount of supersaturation that the tissues can tolerate. This maximum value (or M-value) is the dividing line between having decompression sickness (bubbles) and not having decompression sickness (no bubbles).
Unfortunately, it’s not as simple as that. M-Values have been represented by a solid black line drawn through a fuzzy grey area. This is illustrated, in colour rather than in shades of grey, in the diagram below. At the bottom, with low levels of supersaturation, the diagram is green, indicating no risk of DCS. At the top the diagram is red showing a high risk of DCS. The M-Value is represented as a solid black line drawn across the middle of the area. However, as you can see in the diagram, the black line does not really represent the exact point where the colour switches from green and red as the colour slowly changes from one to the other over a much broader area than that represented by the M-value line. As a result, an ascent from a no-deco dive that goes up to the M-value line or even just close to it risks generating bubbles even though we have not exceeded the M-value.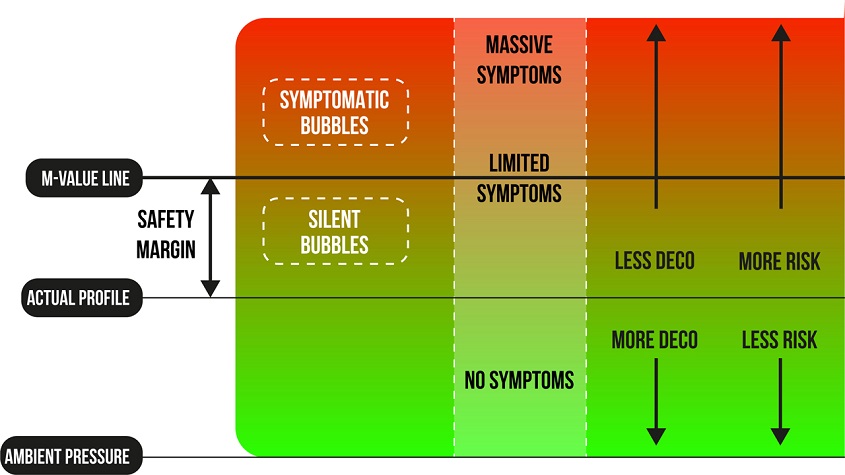
The safety stop allows us to keep a safe distance from the M-value line, as represented by the ‘actual profile’ line on the diagram. This builds in a safety margin by keeping us a distance away from the M-value even during no-stop dives. The value of this was illustrated in a study involving divers carrying out a nitrox dive for 25 min to 36m (120 ft). On the tables they were using this was a no-stop dive. The divers were split into three groups. The first did a direct ascent to the surface at the normal ascent rate but with no safety stop. The second group did the same profile except for a 2min safety stop at 3m (10 ft). The third group again did the same dive but with a 1min stop at 6m (20ft) and a 4min stop at 3m (10ft). None of the divers developed DCS so from that point of view all of the dives could be considered successful. However, the researchers also conducted doppler ultrasound testing on each group of divers. Doppler testing uses ultrasound to detect bubbles within the body. The testing was conducted as soon as the divers surfaced and then at intervals of 15 mins up until 2 hours after the dive.
The results are shown in the graph below. From this we can see that the direct ascent generated a significant number of bubbles on ascent and the bubble count increased 15 minutes after the dive. The count then dropped off slowly over the next 2 hours but there remained a certain number of bubbles in the system even after 2 hours. The second group did a 2-minute stop at 3m (10ft) and you can see that just this 2 min pause had a considerable impact on the bubble count. There were some bubbles on ascent but less than were left on the direct ascent after 2 hours. The number again increased slightly and then dropped off slowly and a relatively small number were left after two hours. The third group, with a 1 min stop at 6m (20ft) and a 4 min stop at 3m (10ft) had fewer bubbles again and these had completely disappeared by 45min.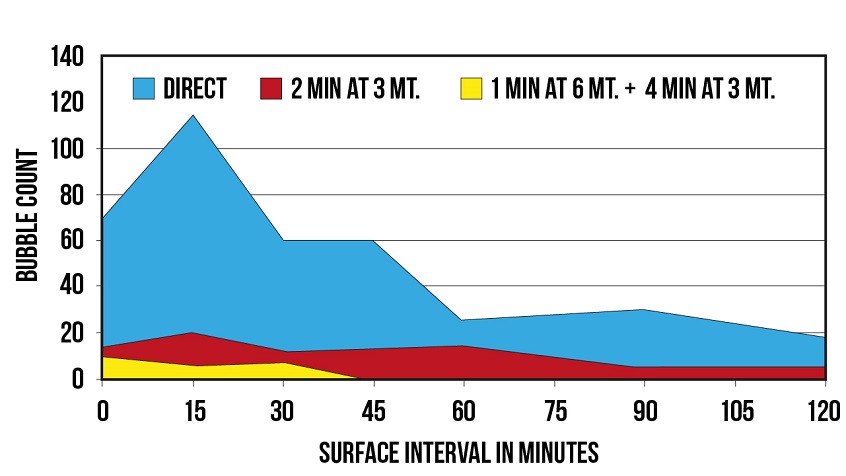
Of course, I said that none of the divers had any signs or symptoms of DCS so we could say that all the dives were successful. However, bubbles detected in this way (known as Venous Gas Emboli or VGE) are considered an indication of ‘decompression stress’. This can be thought of as an indication of potential decompression risk. The second reason why these bubbles are important are that if we are considering a repetitive dive then we may be starting the second dive with bubbles in our system. Divers often leave a surface interval of 1-2 hours between dives. In the case of the direct ascent, even with a 2-hour surface interval, the first group would be starting the second dive with more bubbles than the other groups had immediately on surfacing from the first dive. From this you can see that we might be better off doing a safety stop and just a 45min surface interval then a direct ascent and a 2-hour surface interval.
From this we can see that safety stops make a big difference and can make a significant reduction in decompression stress. Next time a diver misses a safety stop, show them the graph above and explain that they might want to skip the second dive, take an extended surface interval or work on their buoyancy.
MYTH – You must always do a safety stop
Safety stops are a really, really good idea and you should do them whenever possible. However, this sometimes gets phrased as “you MUST ALWAYS do a safety stop”. Given the explanation above this seems like good advice rather than a myth. However, the problem with statements like this is that they get turned into rules and dogma and the original intention behind the rule gets lost and eventually the rule is all that is remembered. The reason for doing a safety stop is to increase safety by reducing our DCS risk. However, if doing a safety stop is likely to increase our risk then the safety stop is defeating the very purpose it was created for. There are times when doing a safety stop can increase our overall risk rather than decrease it. For example, if a diver is running dangerously low on gas, doing a safety stop may then result in an out-of-gas situation. In this case the safety stop has increased the drowning risk much more than it has decreased the DCS risk. In this situation, the safest option would be to not conduct a safety stop. Similarly, if a diver is suffering from a serious medical condition such as a heart attack, Immersion Pulmonary Oedema (IPO) or some other life-threatening condition then insisting on a safety stop is increasing their risk by increasing the time to get the casualty to definitive care.
Situations like this are clearly exceptional situations and it is likely that the majority of divers will never encounter them. Furthermore, running low on gas is something that can be avoided with good gas planning and monitoring. However, there are some things we can never predict and unexpected medical conditions are one such situation. Knowing when your buddy is having a medical emergency and realising that, in this instance, it makes sense to skip a safety stop is a difficult situation to manage. If you have not already taken your rescue course then I would advise signing up for one. It will give you the opportunity to explore these types of problems and talk through the various options.
This situation becomes even more complicated when it comes to mandatory decompression stops. The risk of missing a decompression stop is even higher and normally everything should be done to avoid this. Our gas planning must be comprehensive enough to ensure the team can complete the dive even if one of the divers has a catastrophic loss of gas. However, the risk of unexpected medical conditions is always present. If your buddy is suffering from a heart attack or IPO then keeping them in the water to complete their decompression schedule is probably not the best option. Taking them to the surface would be the best option for them as keeping them in the water is likely to ensure they do not survive. This needs to be balanced against the risk of DCS to yourself. For more information on this I would suggest you have a look at the UHMS Recommendations for rescue of a submerged unresponsive compressed-gas diver.
As we have seen, safety stops are a very effective way of reducing our decompression risk and should be included in any dive where it is practical. However, we have also seen that there may be some very rare situations where it makes sense to skip a safety stop in order to reduce the overall risk of the dive.